
Common Questions About MCL Knee Sprains
March 15, 2017
What is a MCL Sprain?
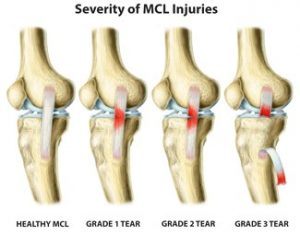
MCL stands for medial collateral ligament and is located on the inside of the knee. The MCL originates on the femur (thigh bone) and inserts on the tibia (large bone of the lower leg). The MCL splits slightly at the knee joint and some fibers also insert onto the medial meniscus (cushion inside the knee). Due to attachment of the MCL on the medial meniscus, MCL sprains may also have an associated medial meniscus tear. An MCL sprain occurs when there is a direct force applied to the outside of the knee, pushing the knee inward. MCL sprains may also occur when a person sustains an ACL (anterior cruciate ligament) tear. There are 3 grades of sprains. A grade one sprain involves stretching and minor tearing of the MCL fibers; a grade two sprain involves partial (50%) tearing; and, a grade three sprain is a complete tear or rupture of the MCL. After sustaining any type of MCL injury, there may be difficulty bending and straightening the knee.
How are MCL Sprains diagnosed?
MCL sprains can usually be diagnosed clinically via physical exam. The health care provider will perform a special test called a valgus stress test. This test may reveal pain and/or instability on the medial side of the knee. X-rays may be ordered which may reveal an avulsion fracture; this involves the MCL pulling a small chip of bone off of the femur. A MRI may be ordered to verify the extent of tearing that has a occurred to the MCL and will also diagnose any additional associated injuries.
How is an MCL Sprain treated?
Most MCL sprains will heal with conservative treatment. These sprains include grade one and grade two sprains. Conservative treatment involves non-weight bearing with the use of crutches until the patient is able to walk without a limp or pain, and physical therapy to strengthen the surrounding musculature (quadriceps, hamstrings, adductors (groin)). The patient may also be placed in a hinged knee brace to help protect the knee from side to side motions. A grade three sprain/tear may require surgical repair.
Why should I consider MCL Surgery?
If someone has a complete tear of the MCL conservative treatment may be an option. The leg would have to be placed in a knee immobilizer, typically locked in full extension, for several weeks to allow scar tissue to form and repair the MCL. After scar tissue has formed, the patient will need to attend physical therapy to strengthen the surrounding musculature. Surgical treatment involves repair of the MCL or reattachment of the ligament to the bone. Surgical repair is not done arthroscopically; it is an open procedure. Surgical repair is preferred for athletes that require excessive amounts of twisting and pivoting at the knee joint.
What are MCL surgery post-surgical restrictions and recovery?
Following MCL surgery, the patient will be placed in a knee immobilizer that is locked in slight flexion (bent knee). The brace can be unlocked at the discretion of the doctor and physical therapist. With the brace locked in flexion, the patient will be non-weight bearing with the use of crutches for 4-6 weeks. The brace can be slowly unlocked to increase range of motion at the knee at the doctor or therapist’s discretion. Once the patient is permitted to weight-bear, strengthening, range of motion, and balance, are key areas that are addressed in therapy. Aggressive therapy usually does not occur until 12 weeks after surgery. It is important to realize that it may take up to a year for a patient to have full recovery following surgical repair of the MCL.
What are the risks of MCL Surgery?
Complications or risks are associated with any surgery. Common risks include: infection, loss of range of motion, and instability. In most cases, the benefits of surgery out weigh the risks.
Written by: Lisa Osterbrock, PA-C, ATC 9/23/14
Edited by: Robert Rolf, M.D.